

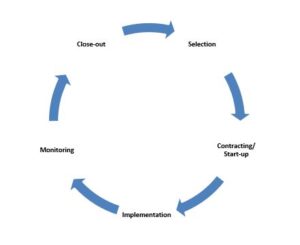
5. Phases in the partnership process
Working in partnerships could be divided into 5 different phases. These phases are coinciding with the moment in the project cycle. The figure below represents the phases in the partnership process for a single project during a rapid onset emergency. In reality however, you may have strategic partners for a longer period beyond the duration of a project.
Ideally, the partnership process is started as part of your preparedness planning. This basically means that the selection process has been completed during “peace” time, resulting in a framework agreement to work with a partner during an emergency. This will save considerable time once an emergency hits. Moreover, identifying partners during your emergency preparedness planning will provide an opportunity to invest in capacity development of the partner. Partners are usually selected before proposal design, but this is not always possible.
Each phase in the process has some critical steps that have to be taken. The exact steps in the partnership process may vary in each response. The reality of an emergency is often complex, hence the below guidelines should be tailored to your specific needs and context. It is recommended however to adhere as much as possible to the specific steps outlined below.
5.1.1 Why is selection so important?
A partner selection process should be objective, transparent and fair. The main reasons for having a proper selection process in place are to:
- Identify the best matching partner and avoid unsuitable partners
- Getting to know potential partners and understand strengths and weaknesses
- Identify potential financial, reputational or security risks for CARE
- Ensure all potential partners have a fair chance and the process is transparent
- Comply with donor and CO rules for procurement or selection of sub-grantees.
5.1.2 Meeting donor requirements
Most COs have sub-granting procedures in place. The selection process during an emergency should always be in line with these procedures as well as with donor regulations. Where possible, these procedures should be simplified and relaxed during an emergency in order to save time.
Partners are usually selected through a competitive bidding process. Occasionally however, they might be appointed (sole-sourced) if there is a good justification to do so. The checklist below lists the standard steps in the selection process.
Selection process Checklist
- Develop eligibility criteria
- Publish a “call for partners”, or approach potential partners directly and invite them to apply
- Short-list applicants by scoring against eligibility criteria
- Visit potential partners and do a quick-organizational capacity assessment
- Conduct reference checks
- Pre-select best partner(s)
- Conduct due diligence assessment (to establish risk rating); only with pre-selected partners
- Conduct Bridger check
- Convene selection committee and make final decision
- Document selection process and justify decisions
5.1.3 Developing eligibility criteria
It is important to know what you are looking for in a partner. Besides, scoring partners against eligibility criteria will increase the objectivity of the selection process. Eligibility criteria may vary depending on the context and specific situation of your response. The following criteria are often considered:
5.1.4 Eligibility criteria
- Proven track record in emergencies: partner has experience working in emergencies
- Proven track record in core sectors: partner has expertise in CARE’s core sectors (sectors of your response strategy)
- Geographical coverage: partner has presence in CARE’s target areas
- Institutional capacity: partner has adequate policies, procedures and systems in place to support the work of the organisation
- Finance & compliance: partner has adequate control mechanisms in place to ensure sound financial management and minimise financial risks
- Scalability: the partner has a balanced portfolio size; it has the ability to absorb more funding in a short time but at the same time is not being overfunded by donors
- Reputation: partner has a good reputation and is well accepted in the communities and areas of operation
- Relations with authorities: partner is seen as a legitimate party – and has good relations with the authorities
- Compatible values & principles: partner has compatible beliefs, values and principles to CARE
- Humanitarian principles: partner is neutral, independent and impartial and is guided by the humanitarian principles
- Partner diversity: the group of CARE’s partners should be a cross section of society, reflecting ethnic as well as possible partisan affiliations
Annex 12.2 – Example Eligibility Criteria Rating Tool
Good practise would be to agree upon criteria prior to publishing a call for partners. The eligibility criteria should be documented and agreed upon by the selection committee.
5.1.5 Capacity assessment
The choice of new partners should usually be confirmed by assessment of suitability, and programmatic, operational and financial capacity. The process also offers an opportunity to discuss expectations and to identify areas where assistance might be useful.
Usually, a short visit (2-3 hours) to a partner is sufficient. Filling out a capacity assessment questionnaire as well as direct observation should be enough to give you a first impression. Assessments can be time consuming so be sure to keep it short. The size of the grant, duration of the program as well as the fact if the partner is known to you, will all determine the length and depth of the capacity assessment.
As an organization whereby gender equality and the empowerment of women and girls is at the center of our work, having gender sensitive partnerships is a priority for CARE. As part of our assessment of partners for value addition, effort should be made to determine the following:
- Does the partner have experience implementing gender sensitive programs?
- Can we work with our partners to build their capacity, or learn from them, in gender sensitive programming?
- Do CARE staff and partners have the attitudes, knowledge and skills they need to interact with marginalized groups such as women?
- Do CARE and partner staff reflects a balanced ratio of male and female staff, including at senior levels?
5.1.6 How to conduct Assessments
Key issues to assess
• Legal status, governance, office locations
• Staffing and management structure
• Capacity to programme: experience, expertise, and size and quality of programmes
• Procedures and staff capacity to manage finances, procurement and logistics
• Amount of funds normally handled and quality of previous reports
• Credibility and reliability-‘reference check’.
Methods and sources
• Explain clearly the purpose of the assessment, to avoid suspicion.
• Interview various partner staff (including program and finance staff).
• Check background documents, financial statements and audit reports.
• Visit project sites and talk to beneficiaries if possible.
• Consult other stakeholders-previous donor, government and local stakeholders.
• Consult INGO colleagues. Do they know of the partner? Do they intend to work with them too? Coordinate to avoid overloading local agencies. Remember, local agencies are sometimes unrealistic about commitments.
The annexes below can serve as a guideline and inspiration to develop your own tool. Your assessment tool should be adjusted to fit your specific context and operations.
Annex 12.3 – Emergency Response Capacity Assessment Tool
5.1.7 Due diligence assessment
Assessments should also consider ‘due diligence’ issues that might make an agency ineligible as a partner. While the context can call for heightened awareness, it is often possible to get enough sense on these from normal inquiries. Concerns can include:
- political affiliation or involvement of the agency and its key officers
- corruption, perhaps indicated by bad bookkeeping, audits or past donors
- nepotism, where key staff have close family links to CARE employees, or where nepotistic hiring clearly compromises the agency’s integrity
- partiality to beneficiaries on grounds such as ethnicity, religion or clan politics
- abuse of power in the field, including for money or sex
- unsuitable mission-for example, a mission to spread religion can be an issue
- links to warring factions or insurgent movements
- links to terrorism-a big issue for some governments and CARE Members.
5.1.8 Terrorism concerns and legislation
Check with your Lead member and relevant donors if there is any requirements related to due diligence or terrorism legislation. Standard procedure for CUSA offices is to conduct a “ Bridger check”. The bridger check will conduct due diligence on fraud, anti-money laundering, foreign corruption and terrorist financing. CUSA offices also often uses a due diligence tool, which is focused on assessing the financial risks of working with a potential partner.
Annex 12.6 – Due Diligence assessment CUSA
While the capacity assessment is focusing on existing capacities, due diligence is focusing on establishing a risk rating. Due diligence (or risk) assessments should only be conducted to pre-selected partners.
5.1.9 Selection committee
Decisions around selection of partners are usually made by a selection committee (partnership committee or Decision Making Committee), which is overseeing transparency and fairness of the selection process, and ultimately has approval authority. The aim of this committee is to objectively review and verify the partner identification and selection process, as well as to address critical challenges related to the partnership over the course of project implementation. Typically, such a committee is chaired by the ACD, and includes relevant program, finance as well as safety & security staff.
Once the partner is selected it is time to agree on the terms and conditions of the partnership. Contract negotiations, as well as starting-up the partnership, can be a lengthy process. It often happens that this process takes too long, causing frustrations and delays in the response. Having a framework agreement in place developed during the EPP, will significantly reduce the time spent in this process. Still, for every individual project, the following steps will need to be done:
Contracting & Start-up Checklist
- Decide on your model of collaboration
- Develop and agree on partner budget
- Develop and agree on partner work plan
- Develop and agree on M&E plan and tools
- Negotiate terms and conditions & sign off partnership agreement
- Transfer 1st instalment to partner
- Conduct inception workshop
The content of a partnership agreement, as well as the accompanying budget and work plan, should be developed jointly. Do not impose anything to your partner. This will only cause a lot of frustration and problems during the implementation stage.
5.2.1 Models for collaboration
A ‘model’ for partnership will describe how much, and in what ways, CARE is to be involved in operations. At one extreme, partners might have great autonomy, while CARE just monitors and receives reports. At the other, CARE can be very hands-on-directing activities; handling procurement, logistics or finances; providing training or mentoring; and participating in day-to-day decisions.
Factors that should inform decisions about the model for collaboration include the capacities of each agency, the programme complexity, the partner’s track record, the degree of trust and the amount of funds. These vary case-by-case. But in general, the smaller the funding, the greater the partner’s capacity; and the more trust CARE has, the more hands-off it can be.
5.2.2 Consider these issues for collaboration
- Whether all aspects of a programme can be implemented by a partner, and whether CARE should conduct some of the activities
- Which functions-procurement, logistics, warehousing or financial-can be managed by partners, and which should be handled by CARE
- Whether CARE should provide TA or training, for example, in programme approaches, standards, finance or procurement
How the relationship will be coordinated and managed-who makes what decisions, how often management meetings take place, etc.
5.2.3 Making and managing budgets
- Agree on budgets before programmes start-negotiating them after the start is more difficult.
- Use formats and budget line descriptions that meet donor/CARE standards.
- Review budgets to ensure all costs are covered, and are not too high or low.
- Be clear on administration/programme split. A split of 40:60 is a common upper limit.
- Pay partner overhead. This is often 5-10% of budgets. If donors won’t pay it (and they often won’t), CARE can agree a split, or find other ways to budget it.
- Be firm. Some see emergencies as an opportunity to submit ‘fat’ budgets.
- Use established partner scales for salary, benefits, per diem and transport, within permitted donor limits. Otherwise, use CARE or common local rates.
- Avoid duplication of project staffing structure between CARE and partner. Remember that CARE is not a direct implementer and has different responsibilities.
- Include simple narrative notes in budgets to explain costs.
- Budget line flexibility should be clear. Establish which budget lines may vary, and by how much. Budget line flexibility is usually around 10%.
- Budget amendment must be governed by contracts. Justification is essential.
- Assign partner costs to a sub-grant account if possible. Otherwise, consider how to manage account codes.
5.2.4 Developing a work plan
- Agree on exact activities, division of responsibilities and timeline. This is the time to get specific and think about the details.
- Be flexible. Particularly during emergencies the situation will change on a daily basis. Hence the work plan may be modified multiple times to reflect the changing situation on the ground.
- Include training sessions and capacity building interventions where relevant.
- Also start working on a procurement plan as soon as numbers and locations are known. Procurement may take a lot of time so the sooner this plan is ready the better.
5.2.5 Develop a M&E plan and tools
- Developing a M&E plan during the contracting/start-up stage ensures the partner is well aware of the M&E standards and obligations.
- Agree on key indicators, data tracking sheets and reporting requirements.
- Keep M&E light, simple and easy to use! Focus on getting essential M&E data only. Complicated tools and heavy M&E protocols are not suitable for emergencies. This can cause delay in program implementation by overburdening the partner with paper work.
5.2.6 Negotiating and signing the Partnership agreement
Consider the following when developing the partnership agreement:
Checklist
- A standard format and conditions should be pre-agreed by senior CO staff (and possibly a lead member representative). If possible, use established formats.
- The conditions of the contract should be discussed and determined jointly with the partner agency. Do not just impose conditions to them.
- Senior staff in finance, support and programme departments should be consulted and approve sections of the contract related to their area of responsibility.
- Approval and sign-off authority for contracts should be clarified in the sub-grant procedures. Usually the size of the grant determines the level of sign-offs.
- Make at least one original copy of the contract each for the partner and for CARE. CARE should hold at least one original in the CO HQ. The project managers must also at least get a copy for reference.
The following is an example of the structure and content of a standard partnership agreement:
- Contract number, date
- CARE/partner name, address, contract manager and key staff if required
- Start & End date
- Goal, objectives and perhaps also more general core values
- The scope of work/cooperation (what, where, when)
- Roles and responsibilities, such as:
- meeting programme standards and adhering to codes of conduct
- ensuring coordination and management
- Organisation-project management, coordination structures
- Amount of grant and eligible expenses
- Disbursements and bank details
- Reporting requirements
- Specific donor requirements (if any)
- Asset and inventory management
- Account keeping and audit
- Methods of dispute resolution, amendment and termination
- General issues-use of name, rights to work, visibility, force majeure, etc.
- Clauses to insure against fraud, corruption, terrorism
- Annexes should include:
- Activities, targets, work plan, budget and disbursement/reporting schedule. These might be in a donor-approved project proposal
- reporting requirements, reporting formats
- Procurement, logistics and financial management rules.
- M&E plan
Annex 12.10 – Sub-grant agreement template CUSA
Annex 12.11 – Sub-grant agreement modification template CUSA
5.2.7 Pre-Authorisation Letter (PAL)
5.2.8 Transferring 1st instalment to partner
Once the partnership agreement is signed off by all parties, the 1st installment should be transferred to the partner. CARE has an obligation to transfer funds to a partner as soon as possible. Delay in transferring funding to the partner can be a huge obstacle in effective program implementation, particularly with partner that have limited pre-financing capacity. The new grant will have to be set-up in the administration systems and this may take some time. Following up on timely installments to partners is a critical task for CARE staff.
5.2.9 Inception workshop
An inception workshop (usually 1 full day) should be organised a soon as budgets and work plans are agreed upon. The workshop is meant to introduce the program to all relevant staff and kick-start implementation. This is the perfect occasion to introduce CARE’s culture and principles, explain specific donor regulations, agree on programming standards, clarify mutual expectations and refine your implementation plans. Typically, staff from programs, finance, procurement as well as safety & security is invited and will organize short sessions.
It is important to realise that the role of CARE in a partnership often has shifted away from direct implementation. This means that the nature of responsibilities of CARE staff will change. The below checklist highlights the main responsibilities of CARE staff in a partnership, where implementation is done by partners.
Implementation Checklist
- Coordination: Conduct frequent coordination meetings with partner staff
- Reporting: Review partner financial and narrative reports
- Disbursements: Ensure timely payments/disbursement due to partner
- Ensuring program quality: Provide technical assistance, on the job coaching and (refresher) training where needed
5.3.1 Partner Coordination
Frequent face to face meetings are important during the implementation stage. Ensure to invest in personal relationships with partner staff. Remember, having good personal relations with partners is one of the critical success factors in a partnership. Foster a climate of trust and openness, so that partners dare to speak out. Particularly in the early stages of a partnership, it may be good to jointly go over the work plan and discuss progress and challenges.
In case of multiple partners working in the same project or geographical area, it might be good to bring partners together in one meeting. Facilitate interaction among partners. Do not forget to use social media (facebook, skypegroups, whatsapp groups) when working with multiple partners. It can greatly improve information sharing and coordination.
5.3.2 Reporting
Progress and finance reporting often present challenges with partners. While falsification and misreporting do occur, more common still are poor presentation of data, irrelevant information, a focus on positive news, and poor analysis of problems and lessons. On the other hand, CARE is often overburdening partners with information requests and reporting requirements. Tips to improve partner reporting include:
Checklist
- Specify the required content and submission dates for reports in contracts.
- Provide sample formats, with guidelines on how to complete them.
- Keep formats clear, short, and easy-to-complete. Don’t ask for lots of information that will be of limited use.
- Minimise the number of reports to essential only. More reporting is not going to lead to improved programming.
- Encourage CARE and partner staff to ‘own’ report formats by developing or modifying them together.
- Discuss how partners will resource for staff to manage data and reporting.
- Plan to provide mentoring or training for partner staff, as appropriate.
- Offer hands-on assistance to make reports if needed. Helping partners to get them right the first couple of times can save a lot of pain later.
- Be clear about who receives reports, how many copies, who proofs, who approves and turnaround times. A memo can be issued to outline these.
- Hold internal review meetings on partner reports with programme and support staff present. This can help to get a holistic view of progress.
- Consider scheduling field monitoring after receiving reports, to verify data.
- Meet partners to review lessons and determine follow up plans.
- Provide partners with feedback from support and programme staff on what is good about their reports, and what can be improved.
5.3.3 Planning and handling disbursements
- Funds are usually disbursed to partners in instalments. This limits financial exposure, as the use of funds is accounted for incrementally.
- The number of tranches depends on CARE’s assessment of risk-the greater the risk, the more instalments there will usually be. More installments mean more work and administration however. Reduce the number of installments where possible.
- Disbursements should depend on adequate progress and financial reports.
- The first tranche of funds is almost always disbursed on contract signing.
- Subsequent instalments are usually disbursed after a certain percentage of the last tranche is used (often 75% or 90%) and adequate reports are submitted.
- A final disbursement (often around 10% of the contract value) is withheld until submission of the final report, audit and resolution of any outstanding issues.
- Paying partners on time is one of CARE’s key obligations, yet delays are fairly common. Internal agreement on roles, documents required, sign-off authorities, and turnaround times will facilitate smooth internal processing.
- Payments to partners are usually accounted for as advances and are cleared on receipt of reports. This can lead to liability and exchange rate losses. Some COs ask donors to expense sub-grants on disbursal, or invoice for the cost of capital.
- Pre-financing by partners makes life easier for CARE, but is often not viable for partners with limited liquidity. It can be unfair to push them to do it.
See also Chapter 17 Finance.
5.3.4 Ensuring program quality
Ensuring that partners meet standards to which CARE is committed to is a tough task. Many have limited knowledge or capacity to implement best practices for activities like distribution, and a weak grasp of issues like Sphere standards, accountability mechanisms and gender sensitive programming. Suggestions to strengthen partner capacities and ensuring program quality include:
Checklist
- Foster common understanding on a programme by holding an inception meeting for CARE and partner staff to discuss standards, the objectives, activities, obstacles, programme management, etc.
- Run training sessions for partner staff at the earliest possible time. Ensure that they are relevant, concise and well targeted, and try to conduct them in the field.
- Provide tools and materials to support training. Preparing translated manuals prior to an emergency is a good practice.
- Follow up on training with field visits, meetings, or refresher courses. This will be much more effective than just one-off events.
- Consider seconding CARE staff to partners to mentor them for a defined period, or arrange for partner staff to learn by shadowing CARE operations.
- Ensure that programme monitoring covers quality and standards issues.
- Budget for partner capacity building interventions in project proposals.
- Give partners access to tools and materials such as the CET

Monitoring Checklist
- Conduct frequent monitoring field visits
- Review and compile M&E data from partner
- Conduct mid-term partnership review (survey)
5.4.1 Monitoring program activities
While monitoring aims to ensure that funds are used in compliance with contracts, it is not meant to be an exercise in ‘policing’ partners. Instead, it is an opportunity for both to learn and improve. Partners often welcome this approach, and some even ask CARE to monitor more, to better understand their challenges. The following is recommended:
- Draft a M&E plan, including clear and simple formats at the start of the project
- Conduct regular monitoring field visits
- If the context does not allow for field visits (e.g. Syria, Afghanistan, and Somalia), use third-party monitoring or contract external consultants. Video live-streaming or social media can provide another solution to keep in touch with partners in remote areas.
- Keep monitoring light and simple. Make sure you are not overburdening your partner with information requests, meetings or visits,
- Listen to partners. Ask proactively for feedback and solutions to challenges. Partners often have great ideas on how to improve programming.
- Make sure to act on feedback, complaints or suggestions that come from partners.
See also Chapter 9 Monitoring and evaluation.
5.4.2 Monitoring the partnership
Monitoring the partnership itself is as important as monitoring program activities. If there are challenges in partnering together, this should be identified and addressed. If issues between the parties are not addressed adequately, this may become an obstacle for responding effectively during an emergency.
Continuous monitoring of the partnership relation therefore is critical. CARE should be open to receiving feedback and complaints and a systematic process needs to be in place to facilitate this and track performance. Some recommendations that could help to monitor and evaluate the partnership itself include:
- Make time during face to face program meetings with the partner to discuss the partner cooperation and ways to improve this
- Appoint 1 focal person within your office (usually the partnership advisor or someone who is not the budget holder of the grant) to function as an “ombudsman” and who hears and investigates feedback and complaints in the interest of the partners.
- Conduct a partnership review/survey (during implementation and after close-out) to understand better and act upon feedback from the partners.
Annex 12.16 – Partnership Survey CARE DK
Each CO may have its own close-out procedures. Make sure to check this with your CO and Lead Member. In general, the following tasks are part of closing out a partnership agreement:
Close out Checklist
- Consider requesting (no)-cost extension if the burn rate is low
- Verify all project activities have been completed
- Consider donating project assets to partner (refer to donor guidelines)
- Review and approve final financial and narrative reports
- Conduct partnership survey evaluation
- Transfer remaining funds/balance
- Archive final records and project documents
- Invite partner to the After Action Review (AAR)
- Recognise and celebrate achievements of the project
- Send close-out letter to partner
- Consider new project with the same partner
Closing out a partnership agreement is a phased process. Identify in an early stage the key activities to ensure there will be a smooth close-out. Closing out a partnership agreement is not the same as closing out the collaboration. If the cooperation was mutually satisfactory, the partnership can continue through a framework agreement (non-project based), or by starting a new partnership agreement for another project.
